

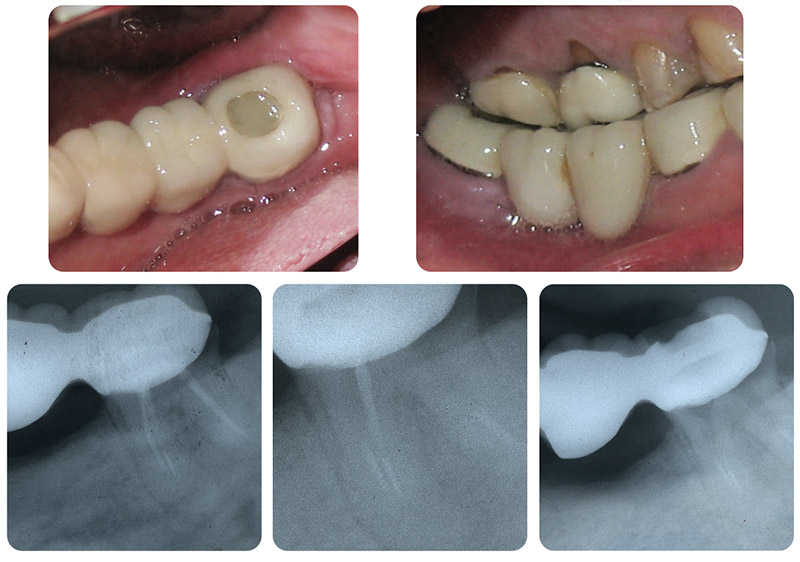
This emergency patient was referred by the concierge at the South Beach Ritz Carlton Hotel. He presented with pain from the lower right area. The clinical and radiographic exam showed the lower right distal molar bridge abutment having been endodontically treated. Careful examination of this radiograph shows a suspicious mesial apical root anatomy ( it would be nice to have a cone-beam tomography image ). This sometimes means that there is an acute apical curvature. The short gutta percha fill may indicate calcified canals.
In order to relieve this patient’s painful symptoms, it would be necessary to remove the obturated gutta-percha to establish drainage. The occlusal composite was removed and access to the pulp chamber was established. At that point an odor was apparent and the patient felt relief.
We also, at that point administered local anesthesia ( topical plus Carbocaine 3 % via a mandibular block ). We utilized small files and chloroform solvent to gently remove the gutta-percha. There was necrotic debris in the distal canal. We were unable to remove all the obturated material from the mesial canals ( the next day when I showed the radiographs to the endodontist next door he immediately advised me that there appeared to be broken instruments in this mesial canal ).
The tooth was left open for drainage. This patient had already started taking antibiotics and I advised him to continue taking this medicine. We also dispensed Vicodin ES a narcotic analgesic.
It is also noted in the photographs that the bridge pontics extend deeply into the muccobuccal fold and are detrimental to proper oral hygiene access
The next day when I called the patient to see how he was feeling, he said he had a lot of pain the first night but now he was better. Follow-up calls for the next few days showed that his pain had subsided. He also told me that he was placing a small piece of cotton in the access hole when he ate and this helped keep the food out.
When I again discussed the case with the endodontist he indicated that this tooth could not be saved. I thought that was interesting coming from a specialist. He advised that the tooth should be extracted and replaced with an implant. From the patient’s point of view, this would be a time-consuming and expensive treatment. If it were my mouth, I would at least attempt to remove the broken instruments and save this tooth.